CASE OF 43 YEAR OLD MALE WITH SEIZURES
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
AFEEFA FARZANA ,7th SEMESTER
Roll no:09
A 43 year old male patient was brought to the casuality on 18 october 2021 at 8:20 pm with
Chief complaints of fever and sudden onset of involuntary movements of right upper limb and right lower limb with frothing present and loss of consciousness 3 times lasting for 5 min.
HISTORY OF PRESENT ILLNESS [HOPI]:
Patient was apparently asymptomatic till 1 day ago .
Then he developed fever which was low grade and decreased on medication.
At 3:00 pm on 17 october 2021 , after he finished having lunch he suddenly developed one episode of Rt sided UL and LL involuntary movements with loss of consciousness for 10 mins, regained spontaneously and he did not talk after that.
After that he had 2 more episodes, each lasting for 2-3 mins, with one episode of vomiting.
He was treated outside with inj Levipil 2g IV/ stat, catheterised and was referred here
PAST HISTORY:
He was born out of a non -consanguinous marriage.
He had weakness in the fingers of right limb since childhood and was diagnosed with poliomyelitis at age 5 yrs studied upto 6th standard and stopped school due to decreased attention and Memory impairment , walked with support and he used to carry out his daily activities with his left hand.
He was given the job of taking care of cattle, till his father expired around 5 yrs back
5 years ago he had angry burst out and used to beat his family members .
He was taken to yerragadda hospital where they prescribed him antipsychotics. Tab. Risperidone 2mg twice daily and Tab. Trihexiphenidryl 2mg once daily. Since then he is on antipsychotics and he had no episodes of anger burst out.
he is not a known case of DM,HTN,TB,asthma
no surgical history
Pallor: Absent
Icterus: Absent
Clubbing; Absent
Cyanosis; Absent
Lymphedenopathy: Absent
Edema; Absent
Temperature- febrile
BP- 140/90 mm of hg
Pulse- 83 bpm
Respiratory Rate- 18
Oxygen saturation- 98% on room air
CVS- S1 S2 +. No murmurs
RS- NVBS. No crepts
ABDOMEN- soft ,not tender, no palpable masses
CNS-
Drowsy but arousable
Speech- no response
GCS- E2 V2 M5



Higher mental functions - cannot be elicited
Motor examination :
RIGHT LEFT
TONE
Upper limb hypotonia hypotonia
Lower limb hypotonia hypotonia
POWER right left
Upper limb 0/5 0/5
Lower limb 0/5 0/5
REFLEXES right left
Biceps - -
Triceps - -
Supinator - -
Knee - -
Ankle - -
Plantar - -
Gait cannot be examined.
Sensory system cannot be examined.
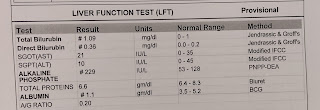
INVESTIGATIONS







ECG :






MRI was done on 18th and 19th. After MRI patient had episode of vomiting.
PSYCHIATRIC REFERAL :




Right side Focal seizures with secondary generalisation .
secondary to bilateral acute infarct in frontal with hemorrhagic transformation with history of psychosis and with history of right sided poliomyelitis
Ryles catheterisation
Inj lorezepam 2 cc/IV/ sos
Inj mannitol 100 ml IV/TID
W/H Antipsychotics
RT feeds- 50 ml milk 2nd hourly.
Day 2:
Inj mannitol 100 ml / IV/ TID
Inj Levipil 1 gm/ IV/ BD
Inj Lorazepam 2 cc/ IV / SOS
RT feeds- 50 ml water 2nd hourly
100 ml milk 4th hourly
Inj Monocef 1g IV/ BD
inj Enoxaparin 40 mg every 12th hourly
Pt was having constant fever spikes (100-101 F) since yesterday night and GCS -3/15 .
No response to deep painful stimulus. pulse rate intially was 52-58 bpm (bradycardia) for sometime.
Later pt had tachycardia with pulse rate of 160-170 Bpm.(sinus tachy) .BP -160/100 mmhg
- INJ PCM 1gm was given twice and tepid sponging ,ice packs were placed. Heart rate decreased to 150 bpm.
At around 4:00 am , pt saturations started falling and spo2 -46% on RA.
Central pulse was present. But there was no spontaneous breathing .
So immediately ambu was done with high flow oxygen. Oral suctioning was done .
After adequate pre-oxygenation , pt was Intubated with 7 mm ET tube and connected to mechanical ventilator .
ACMV VC MODE : RR-14 /min ; FIO2- 100% ;
VT- 480 ml ; peep-5 cm of h20 .
Post intubation vitals : BP- 120/70 mmHg - on NA -6ml/hr
PR- 116 bpm ; regular .
SPO2-. 98% ; RR- 14
CVS -S1S2 PRESENT
RS- BAE present . b/l coarse crepts present.

post intubation ABG :
ABG :
pH - 7.18
Pco2- 59
Po2- 51
SO2- 73.8 %
Hco3- 18.3
POST INTUBATION X ray



Comments
Post a Comment